Poor sanitation, hygiene, and weak healthcare systems were the pillars of argumentation for Tedros Ghebreyesus6 and Melinda Gates7, who wrongly predicted a higher impact of COVID-19 in Africa than anywhere else. Their logic seemed reasonable, with historical examples of diarrheal and other hygiene-related maladies8. However, they overlooked several variables such as immunity, weather, and the leaders’ commitment to the World Health Organization guidelines1,9. Poor sanitation was not initially a major problem because COVID-19 entered Mozambique through people from the upper classes who came from European countries or South Africa, had access to the best sanitation, and had little contact with the “common” population 10, transmitting to few people. Eventually, the disease reached crowded areas with poor hygiene practices such as markets11,12, and only then, sanitation became a significant issue.
The current study aims to validate that population density and access to sanitation are among the variables influencing the dissemination of COVID-19 in Mozambique. In addition, the results will provide support to health personnel, policy-makers, and scholars who need to understand better the pattern of dissemination of COVID-19 in Mozambique and countries with similar natural and social settings.
MATERIAL AND METHODS
Mozambique (10°27’S and 26°52’S;30°12’E and 40°51’E) is a country on the southeastern coast of Africa (Map 1), bordered by the Indian Ocean (east), Tanzania and Malawi (North), Zambia and Zimbabwe (West), South Africa, and Eswatini (southwest)13. The population is approximately 27,909,798, with 28.7 inhabitants/km2 as density14. Mozambique has ten provinces plus the capital and largest urban area, Maputo City (considered a province), located in the southern area 15.
By 2015, approximately 46% of the population lived below the poverty line (US $1.9 purchasing power parity), and 40% had access to improved sanitation16. Limited access to sanitation is among the causes of Cholera17 and other hygiene-related diseases18, certainly increasing the risk of COVID-19 among the Mozambican population. According to World Bank Group16, only 14% of the population below the poverty line and 42% above it had sanitation facilities in 2015.
 |
Map 1 - Mozambique. Source: Library of Congress19, under public domain.
Data retrieval and analysis
The data was retrieved the data on 11 February 2021:Mozambican population density (in inhabitants/km2) per province from Census 2017 report 20 and data on the percentage of the population with access to sanitation facilities per province in the Mozambique Public Expenditure Review 201421, and the number of confirmed cases from the Ministry of Health’s COVID-19 daily bulletin number 33222. JASP 0.13.1.0 (University of Amsterdam, Amsterdam, The Netherlands, 2020) computed Pearson correlations. Microsoft Excel 2016 (Microsoft Corporation, Washington DC, USA, 2016) was used to perform curve fitting between the number of confirmed cases of COVID-19 and the other two variables and analyze the determination coefficients. Maputo City was included in the study because it is administratively a province.
Table 1 - Mozambique’s provinces, population densities, percentage of people with access to sanitation facilities, and the number of COVID-19 confirmed cases by 8 February 2021
|
Province |
Density (inhabitants/km2) |
People with access to sanitation facilities (%) |
COVID-19 confirmed cases |
|
Maputo City |
3,131 |
73 |
21,828 |
|
Maputo Province |
87 |
46 |
7,236 |
|
Gaza |
19 |
32 |
2,646 |
|
Inhambane |
22 |
17 |
2,469 |
|
Manica |
31 |
20 |
1,724 |
|
Sofala |
33 |
22 |
2,576 |
|
Tete |
27 |
17 |
1,528 |
|
Zambézia |
49 |
6 |
2,641 |
|
Nampula |
73 |
21 |
1,617 |
|
Cabo Delgado |
28 |
6 |
1,976 |
|
Niassa |
14 |
28 |
1,549 |
Sources: Maunze et al. 20, The World Bank Group 21, and Ministério da Saúde 22.
As Figure 1 shows, the number of COVID-19 confirmed cases showed significant Pearson correlations with the population density (p = 0.037) and the percentage of people with access to sanitation (p = 0.031). However, both correlations did not differ much in value.
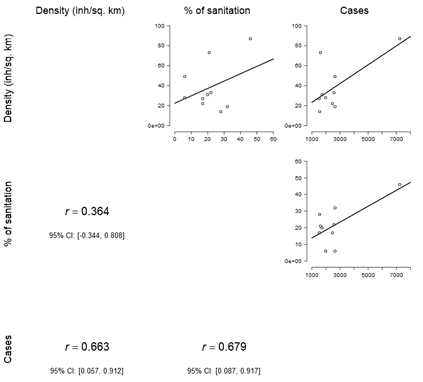 |
Figure 1. Correlation matrix between population density, percentage of people with access to sanitation, and the number of confirmed cases by 8 February 2021 in Mozambique. Note: inh/sq. km = inhabitants/km2; % of sanitation = percentage of people with access to sanitation.
The density did not seem related to the percentage of people with access to sanitation, reinforcing the idea that these variables had an independent impact on the number of cases. This independence is essential because both variables could be “two sides of the same coin,” i.e., one could be affecting the other as the root of the impact both present on the number of cases. Thus, only one would be enough to perform the analysis from this point forward.
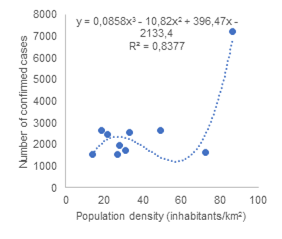
Figure 2 presents the result of a fitting analysis showing the simplest algebraic curves representing how de values population density and the number of people with access to sanitation facilities can serve as predictors of the number of confirmed cases by 8 February 2021 in Mozambique. Both independent variables presented strong coefficients of determination (R2 > 0.5).
 |
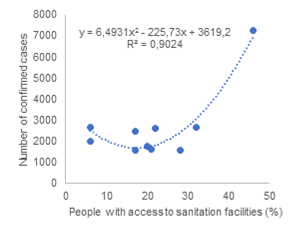 |
Figure 2. Regression analysis of the number of confirmed COVID-19 cases as a function of (a) population density and (b) percentage of people with access to sanitation in Mozambique.
The curve of population density and number of cases presented some consistency (R2 = 0,84) with a cubic function, being such regression more complex than the square function (with R2 = 0,9) between access to sanitation and the confirmed cases. From this data, access to sanitation seems to be a more reliable predictor of the number of cases, although this curve’s shape seems counterintuitive, an aspect discussed in the following section.
Discussion
The results suggested that the number of COVID-19 confirmed cases present positive correlations with population density and the percentage of people accessing sanitation in Mozambique. Furthermore, as predictors of the number of cases, the population density showed a relationship consistent with a cubic function, and the access to sanitation presented a quadratic curve. In advance, it is essential to know that the literature presents plenty of studies about the impact of population density on the number of cases of COVID-19 but not as frequently discussing the relationship between access to sanitation and the pandemic.
Maputo City, its considerably dense population, high access to sanitation facilities, and many COVID-19 confirmed cases. As the capital, Maputo City is the country’s most developed and arguably the busiest area, with people arriving every day from all over the country to study or search for labor opportunities, and it is among the main entry points for people coming from abroad. As mentioned in a previous study 9, the city’s features turned it into a “hotspot” of COVID-19 dissemination since the pandemic entered the country. Due to the New Year-related events, the situation worsened in Maputo City, with many tourists from South Africa and the weak enforcement of COVID-19 preventive measures23. Other areas were also busy, had New Year parties, and received tourists, but not likely as much as Maputo City. Thus, the city was the “stage” of a unique situation for peculiar reasons.
The correlation cubic regression analyses reinforced the idea that population density influences COVID-19 cases in Mozambique. The correlation suggested that, from a simplistic perspective, the intuitive idea that the more people live in a particular area, the more susceptible it is for COVID-19 dissemination. More than intuitive, there is evidence backing up the idea 3,24,25. Some studies did not find enough evidence to conclude that population density affects COVID-19 spreading 2,4, but they resulted from early analyses when data was insufficient to find consistent patterns The impact of density on disseminating the pandemic compares to a network of pipes and tanks as water runs through it. In the beginning, water is more abundant in the source, but it takes the system’s shape as it fills, and in the end, it is more abundant in the tanks. By the same logic, highly populated areas imply more encounters among people, thus, more occasions for COVID-19 transmission. Still, the relationship between density and the number of cases seemed more complex, more easily represented through a cubic function. This complex relationship might result from other factors such as weather9, reinforcement of methods to control the pandemic, and the pattern of migration or people’s behavior1. Several correlation-based and linear regression-based studies analyze the influence of population density on the pandemic, but they do not search for algebraic functions that had better represent such influence.
To the best of the author’s knowledge, the only peer-reviewed study published (locally) in Mozambique about the influence of density on the number of COVID-19 cases, by Arnaldo et al.5, assumed a relationship between the variables, arbitrarily using the idea for further analyses. The authors aimed to predict the risk of COVID-19 dissemination based on different variables, including population density. However, they had no clear information on how severely density could affect the number of cases, resting their proposition on speculation. The current study attempts to clarify and provide statistical support to Arnaldo et al.5.
Regarding how access to sanitation facilities affected the number of confirmed cases, the result seemed counterintuitive, i.e., more people with access to sanitation should imply more hygiene and fewer cases of COVID-19. There are some possible explanations: (1) the country’s more developed areas have more people with access to sanitation, but are also the busiest, where the disease can spread more easily; (2) people with limited sanitation facilities tend to value more such resources, using more adequately. Ekumah et al.26 collected data on access to sanitation and the number of COVID-19 cases in 25 countries of Sub-Saharan Africa, including Mozambique, but their overall result indicate that lack of sanitation, combined with lack of clean water and food storage, is associated with a higher level of violation of lockdown regulations, and a higher risk of COVID-19. The authors analyzed the issue at an international level, thus using data biased due to differences in COVID-19 emergency or lockdown policies and other social and natural factors. Ha et al.27 and Amaechina et al.28 also discussed the importance of sanitation for COVID-19 prevention, but they were more concerned about policies to facilitate the distribution of water and sanitation facilities. Thus, this might be the first study analyzing at a country level how the sanitation coverage affected the cases of COVID-19. Perhaps time will allow gathering more robust data to understand the phenomenon, but so far, it is crucial to persuade the population in densely inhabited areas to abide more responsibly by COVID-19 preventive measures, particularly hygiene.
Future studies shall revisit how COVID-19 dissemination in Mozambique relates to population density, access to sanitation, and include other variables such as the access to healthcare services and the variables mentioned in the paper about the “African miracle” 1: level of implementation of the Strategic Preparedness and Response Plan29 and other guidelines from the World Health Organization (WHO), population migration patterns, the dynamics and management of other illnesses, population age profile, immunity, and vaccination.
CONCLUSION
The study suggests that the number of COVID-19 cases is directly proportional to population density and sanitation access. The correlations were significant (p < 0.05) and high enough to admit their strength (r > 0.5). Fitting analysis showed consistency with algebraic curves representing the predictability of COVID-19 confirmed cases through the population density (cubic function) and access to sanitation in percent (square). More important than understanding a phenomenon is to reason on what to do about it. In this case, population density is a good tool for predictions and decision-making. Knowing how density affects COVID-19 dissemination allows one to understand the spatial pattern of the number of cases throughout the country if the situation does not change. Regarding sanitation, the mere availability of facilities is not enough to ensure the control of COVID-19. It is also essential to promote good hygiene practices and strict fulfillment of the Government’s recommendations.
REFERENCES
1- Cambaza EM. The African miracle: why COVID-19 seems to spread slowly in Sub-Saharan Africa. Revista Científica da UEM: Série Ciências Biomédicas e Saúde Pública 2020; Preprint: 1-8.
2- Bhadra A, Mukherjee A, Sarkar K. Impact of population density on COVID-19 infected and mortality rate in India. Modeling Earth Systems and Environment 2021; 7(1): 623-9.
3- Coşkun H, Yıldırım N, Gündüz S. The spread of COVID-19 virus through population density and wind in Turkey cities. Science of The Total Environment 2021; 751: 141663.
4- Sun Z, Zhang H, Yang Y, Wan H, Wang Y. Impacts of geographic factors and population density on the COVID-19 spreading under the lockdown policies of China. Science of The Total Environment 2020; 746: 141347.
5- Arnaldo C, Arau A, Hansine R, et al. Características sociodemográficas e risco de transmissão da COVID-19 em Moçambique. Revista Moçambicana de Ciências de Saúde 2020; 6(1).
6- Houssin D, Ghebreyesus TA, Yang, Keaton J, Lanche J, Kupferschmidt K. WHO Emergencies Coronavirus Emergency Committee Second Meeting, 30 January 2020. In: Lindmeier C, editor. Coronavirus Disease (COVID-2019) Press Briefings. Geneva, Switzerland: World Health Organization; 2020.
7- Gates M. Melinda Gates: COVID-19 will be horrible in the developing world. In: Harlow P, editor. CNN Business. Atlanta, GA, United States: Cable News Network (CNN), Turner Broadcasting System, Inc.; 2020.
8- Hessel L. The initiative against diarrheal and enteric diseases in Africa and Asia: The role of field actors to successfully address the fight against cholera. International Journal of Infectious Diseases 2014; 21: 112.
9- Cambaza E, Viegas G, Cambaza C, Mongo E. Relevância das condições meteorológicas para a ocorrência da COVID-19. Revista Moçambicana de Ciências de Saúde 2020; 6(1): 15-20.
10- Chongo AE, Sineque AR, Augusto O, et al. COVID-19 reproduction rate: relevance in the Mozambican context. Revista Científica da UEM: Série Ciências Biomédicas e Saúde Pública 2020; Preprint: 6.
11- Macaza BS. Avaliação da qualidade e segurança microbiológica de alimentos de rua vendidos nos mercados municipais da cidade de Nampula, Moçambique. Porto, Portugal: Universidade do Porto; 2017.
12- Manhique GA. Avaliação das condições higiênico-sanitárias e contaminação microbiológica de alimentos, manipuladores e utensílios utilizados na preparação de alimentos em mercados e nas ruas de Maputo, Moçambique. Porto Alegre, Brazil: Universidade Federal do Rio Grande do Sul; 2020.
13- Agulhas and Somali Current Large Marine Ecosystems. National Marine Ecosystem Diagnostic Analysis. Mozambique. New York, United States: Global Environment Facility (GEF), 2012.
14- Instituto Nacional de Estatística. Censo 2017: IV Recenseamento Geral da População e Habitação. Maputo, Mozambique: Gabinete do Presidente, Instituto Nacional de Estatística, 2017.
15- Cambaza EM. The Double Burden of Malnutrition since the Beginning of the Millennium in Adults from Maputo City. Crawley, Western Australia: The University of Western Australia; 2013.
16- World Bank Group. Mozambique poverty assessment: “strong but not broadly shared growth”. Washington, DC, United States: World Bank Group, 2018.
17- Cambaza EM, Mongo E, Anapakala E, Nhambire R, Singo J, Machava E. An update on cholera studies in Mozambique. In: Bacha U, Rozman U, Turk SŠ, eds. Healthcare Access - Regional Overviews. London, UK: IntechOpen Limited; 2020: 1-20.
18- Chissaque A, de Deus N, Vubil D, Mandomando I. The epidemiology of diarrhea in children under 5 years of age in Mozambique. Current Tropical Medicine Reports 2018; 5(3): 115-24.
19- Library of Congress. Mozambique. 1995. https://picryl.com/media/mozambique-1 (accessed 1 March 2021 2021).
20- Maunze XH, Dade A, Zacarias MdF, et al. IV Recenseamento Geral da População e Habitação, 2017: resultados definitivos – Moçambique. Maputo Mozambique: Instituto Nacional de Estatística, 2019.
21- The World Bank Group. Mozambique public expenditure review: addressing the challenges of today, seizing the opportunities of tomorrow. Washington, D.C., United States: The World Bank Group, 2014.
22- Ministério da Saúde. Boletim Diário COVID-19. In: Departamento de Saúde Pública, editor. Maputo, Mozambique: Ministério da Saúde; 2020. p. 2.
23- Nyusi J. Balanço da implementação das medidas decretadas no contexto da declaração da situação de calamidade pública, no âmbito da pandemia do coronavírus – COVID-19. Maputo, Mozambique: Presidência da República, 2021.
24- Kodera S, Rashed EA, Hirata A. Correlation between COVID-19 morbidity and mortality rates in Japan and local population density, temperature, and absolute humidity. 2020; 17(15): 5477.
25- Kadi N, Khelfaoui M. Population density, a factor in the spread of COVID-19 in Algeria: statistic study. Bulletin of the National Research Centre 2020; 44(1): 138.
26- Ekumah B, Armah FA, Yawson DO, et al. Disparate on-site access to water, sanitation, and food storage heighten the risk of COVID-19 spread in Sub-Saharan Africa. Environmental Research 2020; 189: 109936.
27- Ha YP, McDonald N, Hersh S, Fenniri SR, Hillier A, Cannuscio CC. Using informational murals and handwashing stations to increase access to sanitation among people experiencing homelessness during the COVID-19 pandemic. American Journal of Public Health 2020; 111(1): 50-3.
28- Amaechina E, Amoah A, Amuakwa-Mensah F, et al. Policy note: policy responses to ensure access to water and sanitation services during COVID-19: snapshots from the Environment for Development (EfD) network. Water Economics and Policy 2020; 06(04): 2071002.
29- World Health Organization. 2019 Novel Coronavirus (2019-nCoV): Strategic Preparedness and Response Plan. Geneva, Switzerland: World Health Organization, 2020.
RACSAÚDE
Revista Angolana de Ciências da Saúde / Angolan Journal of Health Sciences
ISSN (Online): 2789 - 2832 / ISSN (Print): 2789 - 2824
Equipa Multidisciplinar de Docentes e Investigadores Nacionais (Angola)
Rua Craveiro Lopes S/N, Bairro de Fátima Urbano, Edifício do Hospital Sanatório